How to write a SOAP note with examples for medical students is a core skill in clinical education. It helps you organize patient information. It improves communication with supervisors. It also supports safe patient care. Many students feel nervous at first. That is normal. With practice the process becomes clear and logical.
A SOAP note is a structured way to document a patient encounter. SOAP stands for Subjective Objective Assessment and Plan. Each part has a specific role. When written well it tells the full patient story. This guide explains each section in detail. It also includes clear examples written in simple language.
Understanding the Purpose of a SOAP Note
A SOAP note is more than an assignment. It is a professional clinical document. Doctors nurses and other health workers use it daily. It allows everyone on the care team to understand the patient condition quickly.
For medical students the SOAP note teaches clinical thinking. It trains you to listen carefully. It helps you separate facts from opinions. It also shows how to connect symptoms with diagnoses and treatment plans.
A good SOAP note is clear and concise. It avoids unnecessary words. It focuses on relevant details. It follows a logical flow from patient complaint to plan of care. When you master this format you build confidence in clinical settings.
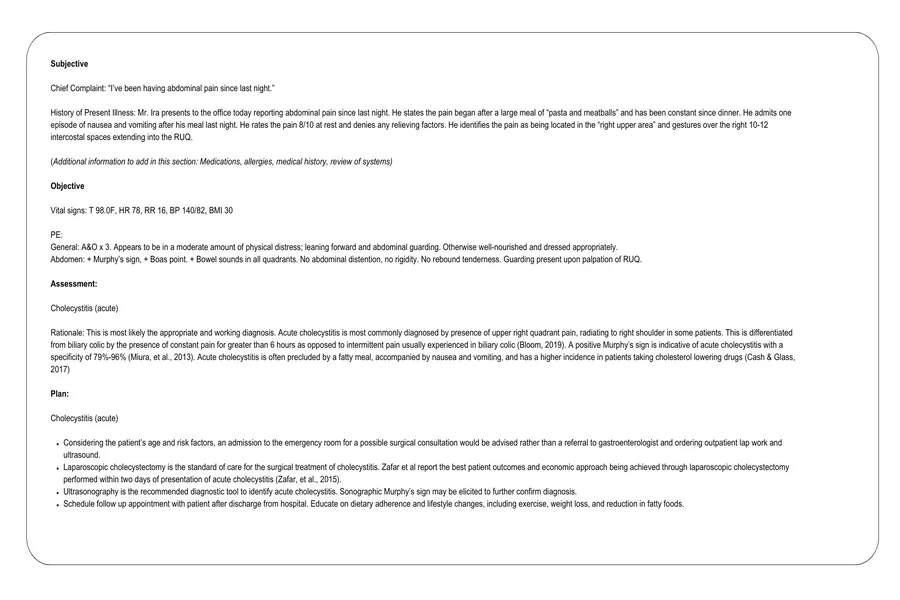
How to Write the Subjective Section Correctly
The subjective section captures what the patient says. It reflects the patient perspective. This part includes symptoms concerns and history as reported by the patient or caregiver.
You start with the chief complaint. This is the main reason for the visit. It should be written in the patient own words when possible. Then you add the history of present illness. This explains when the problem started. It also explains what makes it better or worse.
You may include past medical history if relevant. Medication history and allergies are often included. Social history may be added when it affects care. Always focus on information related to the current problem.
Example of a subjective section
The patient is a 45 year old male who presents with chest pain for two days. He reports the pain started suddenly while walking. He describes it as a tight pressure in the center of his chest. The pain increases with exertion and improves with rest. He denies nausea or vomiting. He has a history of hypertension and takes medication daily.
Writing the Objective Section With Accuracy
The objective section includes measurable data. This part contains what you observe and measure. It does not include opinions or interpretations.
Vital signs are usually listed first. This includes blood pressure heart rate respiratory rate and temperature. Physical examination findings come next. These should be organized by body system. Lab results and imaging findings are also included when available.
Use clear medical terms. Be specific. Avoid vague descriptions. Do not explain what the findings mean here. That comes later.
Example of an objective section
Blood pressure is 150 over 95. Heart rate is 92 beats per minute. Temperature is normal. The patient appears alert and in mild discomfort. Cardiovascular exam reveals regular rhythm with no murmurs. Lungs are clear to auscultation. No edema noted in extremities. ECG shows normal sinus rhythm.
Developing a Strong Assessment Section
The assessment section is where clinical reasoning appears. This is often the hardest part for medical students. Here you analyze the information from the subjective and objective sections.
You list the most likely diagnosis first. You may also include differential diagnoses. Each diagnosis should be supported by findings already mentioned. Keep this section focused and logical.
Do not introduce new data here. Use what you have already documented. Be clear and confident but realistic. It is acceptable to note uncertainty when appropriate.
Example of an assessment section
Chest pain likely related to stable angina given exertional nature and relief with rest. Hypertension is uncontrolled and may be contributing to symptoms. Acute myocardial infarction is less likely at this time due to normal ECG and stable vital signs.
Creating a Clear and Safe Plan Section
The plan section outlines what you will do next. It is action oriented. This part often includes tests treatments medications and patient education.
Plans should be specific. Each problem listed in the assessment should have a corresponding plan. You may also include follow up instructions.
For students this section shows your understanding of management. Always consider safety and guidelines. When unsure state that you will discuss with a supervisor.
Example of a plan section
Order cardiac enzymes to rule out acute coronary syndrome. Start aspirin therapy as indicated. Adjust antihypertensive medication to improve blood pressure control. Advise patient to avoid strenuous activity. Arrange cardiology referral. Educate patient on warning signs and when to seek emergency care.
Common Mistakes Medical Students Should Avoid
Many students make similar errors when learning how to write a SOAP note with examples for medical students. One common mistake is mixing sections. For example adding opinions in the objective section. Another mistake is including too much irrelevant detail.
Using unclear language is also common. Short clear sentences are better. Avoid copying and pasting without understanding. Each note should reflect the specific patient encounter.
Spelling and grammar matter. A SOAP note is a legal document. Review your work before submission. Ask for feedback from instructors. Improvement comes with practice.
Final Thought
Learning how to write a SOAP note with examples for medical students is an essential step in becoming a competent clinician. It may feel challenging at first but it builds a strong foundation for patient care. Focus on clarity accuracy and logical thinking. Practice regularly and review real cases. Over time writing a SOAP note will become a natural part of your clinical routine.